After
achieving a major triumph over Polio, India has touched yet another milestone
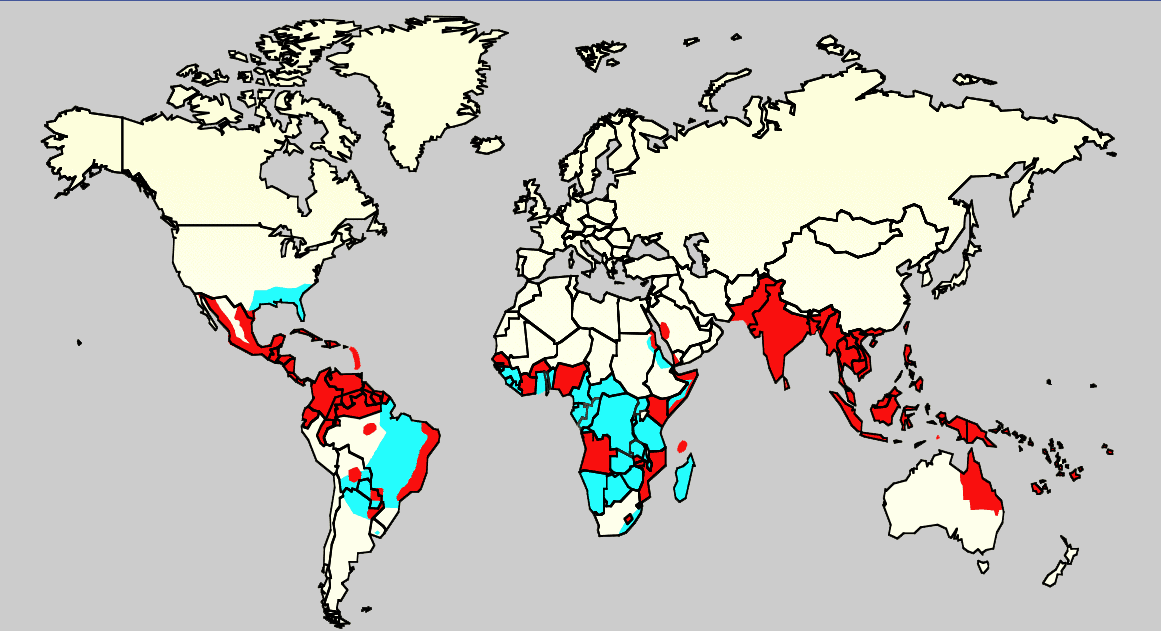
in the public health system. India now lists in the countries that have
successfully eliminated maternal and neonatal tetanus. Maternal and neonatal
tetanus is reduced to less than one case per 1000 live births in the entire
country.World Health Organization declared India
free of maternal and neonatal tetanus on the 15th of May. Nagaland being the
last state to achieve this as validated by a survey conducted in April.

This
remarkable achievement is the part the Maternal and Neonatal Tetanus
Elimination Initiative launched by UNICEF, WHO and UNFPA in 1999, to combat the
deadly spread of tetanus amongst mothers and newborns (due to the unhygienic
conditions of delivery exposing mother and newborns to the toxic bacteria). According
to WHO, over the past 15 years, the worldwide death rate from tetanus dropped from around
800,000 deaths in 2000 to under 50,000 this year. However, in
countries like, Afghanistan, Pakistan and Nigeria, the disease still represents
a public health threat.
India’s victory in the battle
India’s
various national immunization programme and the special immunization weeks helped
in a big way in achieving this milestone. Needless to mention that the most
recent ‘Mission Indradhanush’, helped ensure that children are immunized
against diphtheria, pertussis, tetanus, childhood tuberculosis, polio,
hepatitis B and measles from 60% to 95% and pregnant women are reached with
vaccines.
According to UNICEF, what
made India’s program stand out is the fact that it didn’t rely purely on
immunization drives. Childhood vaccinations were supported with a policy that
encouraged women to give birth in sanitary environments: the Indian government
offered a payment of $21 for every delivery in a hospital, and women who
insisted on a traditional delivery at home were offered free sterilized
delivery kits.
The
‘National Rural Health Mission’ promoted institutional deliveries with a focus
on the poor. The ‘JananiSurakshaYojana’ encouraged women to give birth in a
health facility. With India’s achievement, almost the entire WHO South-East
Asia Region, barring a few districts in Indonesia, has now eliminated maternal
and neonatal tetanus.
Still a long way!
No
doubt, we have reached our goal of achieving maternal and neonatal tetanus, however,
there is still much to be done. Unlike smallpox and polio, tetanus cannot be eradicated,
as tetanus spores remain stubbornly present in the environment worldwide. As
the risk of tetanus persists, we need to continue our efforts to ensure that
MNTE is maintained - women and children are immunized and clean deliveries and
proper cord care activities get a further boost.
Image source:
Image source:




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}